Warren at the CRS provided all values after the first 3.
From the CR societyMatthew Lake (myself)
Total : 3.7 (144mg/dl)
HDL: 1.5 (59mg/dl)
LDL: 1.9 (74mg/dl
Triglycerides: 0.6 (53mg/dl)
Arturo
Cholesterol 100mg/dl
Triglycerides 61
HDL 50
VLDL 12
LDL 38
Willie
Total Cholesterol: 150 mg/dl
HDL: 54 mg/dl
LDL: 80 mg/dl
Triglycerides: 79 mg/dl (
Saul [Zone diet]
Item Value Range
------------ ----- ------
Triglycerides 23 < 200
Direct HDL 81 > 35
Fast Tri/HDL Ratio 0.28 < 2.0
-------------------------------------------
Dean [Zone diet]:
Item Value Range
------------ ----- ------
Triglycerides 49 < 200
Direct HDL 68 > 35
Fast Tri/HDL Ratio 0.72 < 2.0
[Previous to CR, ratio value was ???].
-------------------------------------------
Saul [Zone diet]:
Item Value Range
------------ ----- ------
Triglycerides 35 < 200
Direct HDL 74 > 35
Fast Tri/HDL Ratio 0.47 < 2.0
[Previous to CR, ratio value was ???].
-------------------------------------------
Warren [Zone diet]
Item Value Range
------------ ----- ------
Triglycerides 33 < 200
Direct HDL 54 > 35
Fast Tri/HDL Ratio 0.61 < 2.0
[Previous to CR, ratio value was 2.38].
-------------------------------------------
Khurram [Zone diet]
Item Value Range
------------ ----- ------
Triglycerides 39 < 200
Direct HDL 53 > 35
Fast Tri/HDL Ratio 0.74 < 2.0
[Previous to CR, ratio value was 1.79].
-------------------------------------------
Phil [Zone diet]
Item Value Range
------------ ----- ------
Triglycerides 45 < 200
Direct HDL 92 > 35
Fast Tri/HDL Ratio 0.49 < 2.0
[Previous to CR, ratio value was 2.67].
--------------------------------------------
Michael [Walford diet]
Item Value Range
------------ ----- ------
Triglycerides 49 < 200
Direct HDL 74 > 35
Fast Tri/HDL Ratio 0.66 < 2.0
[Previous to CR, ratio value was 7.52 (316/42)].
--------------------------------------------
Greg [Zone diet]
Item Value Range
------------ ----- ------
Triglycerides 55 < 200
Direct HDL 71 > 35
Fast Tri/HDL Ratio 0.77 < 2.0
[Previous to CR, ratio value was ???].
--------------------------------------------
Larry [Zone diet]
Item Value Range
------------ ----- ------
Triglycerides 67 < 200
Direct HDL 101 > 35
Fast Tri/HDL Ratio 0.66 < 2.0
[Previous to CR, ratio value was 2.06 (128/62)].
--------------------------------------------
Larry [Zone diet]
Item Value Range
------------ ----- ------
Triglycerides 69 < 200
Direct HDL 108 > 35
Fast Tri/HDL Ratio 0.64 < 2.0
From Fontana study
Long-term calorie restriction is highly effective in reducing the risk for atherosclerosis in humanshttp://www.pubmedcen...bmedid=15096581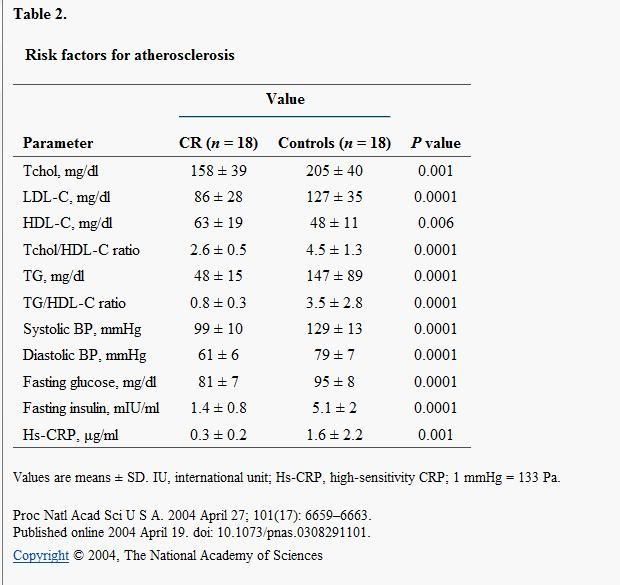
Edited by Matt, 14 October 2008 - 10:58 PM.


























































{kind=link}